
Rhode Island Dual Diagnosis Treatment: The Missing Link in Lasting Recovery
You may be surprised to learn that 41.2% of the 21.2 million adults living with co-occurring disorders and substance use disorders did not receive any substance use or mental health treatment. They never denied help. In reality, the system they wanted to get into wasn’t built to satisfy both conditions at once.
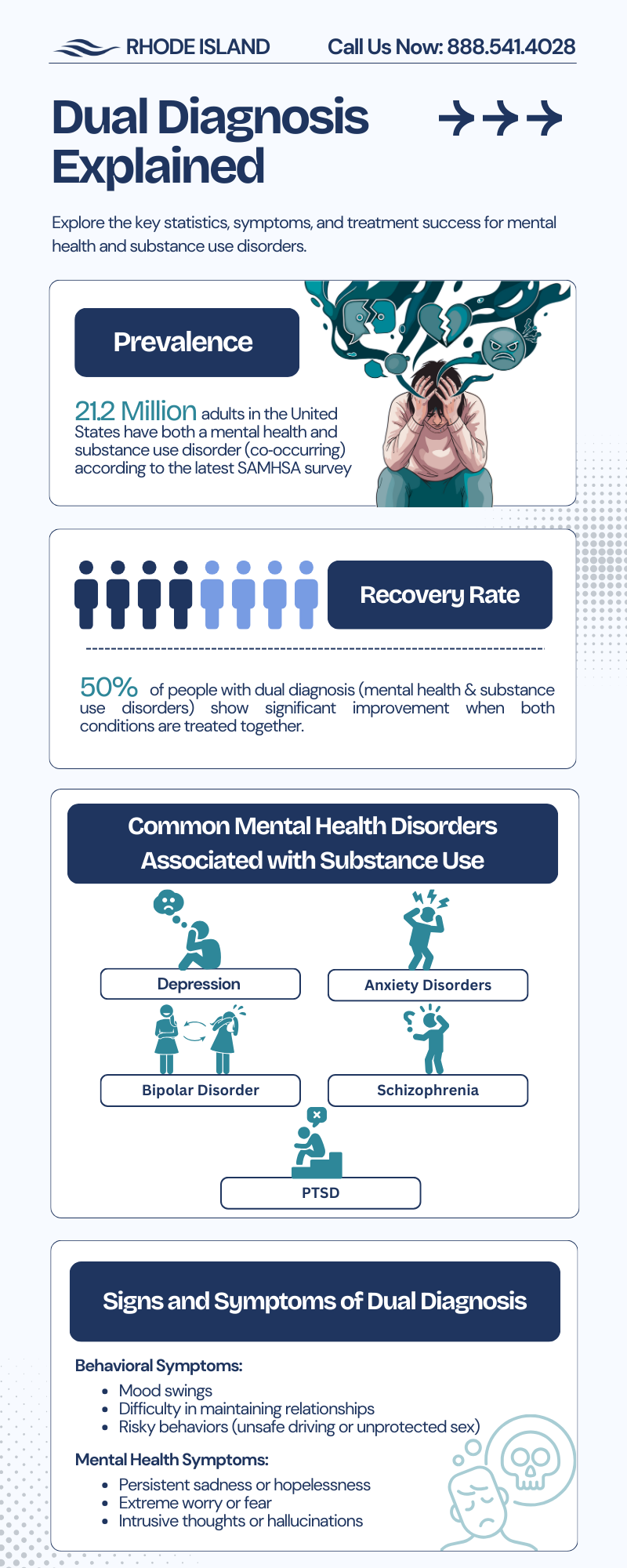
Are you struggling with addiction and depression, PTSD, anxiety, or something you can’t name yet? This article explores what makes good dual diagnosis treatment in Rhode Island and what makes it work or fail.
Dual Diagnosis: An Infinite Loop
The unexpected collaboration between a mental health condition and a substance use disorder was officially recognized as a dual diagnosis in the 1980s. It doesn’t manifest sequentially. Not “first I’ll get sober, then I’ll work on the depression.” Rather, at the same time, because that’s how they operate.
One feeds the other. PTSD drives substance use because substances quiet the noise that trauma makes. Substances worsen depression because they borrow relief from tomorrow and charge interest. Depression almost guarantees relapse because it takes away the reasons to stay sober. 30 to 60 percent of people with PTSD are reported to have a co-occurring drug or alcohol use disorder.
The self-medication hypothesis, the notion that people use substances to cope with distressing trauma symptoms, has received the most empirical support of any explanation for why these two conditions travel together.
The clinical message is simple. Treating only the addiction without addressing the underlying mental health condition isn’t treatment. It’s postponement.
Why “Treating Both” Is Harder Than It Sounds
Most facilities will tell you they treat co-occurring disorders. That’s often true at the clinical level. They have a psychiatrist, offer therapy, and handle medication-assisted treatment. Unfortunately, fewer facilities in Rhode Island have a clear answer for what happens when a patient leaves inpatient and goes back to the life they came from.
Providence ZIP codes had some of the highest eviction rates in the state, about 14.2 per 100 residents from 2021 to 2023, along with Cranston, Pawtucket, and Woonsocket. Moreover, the state’s highest concentration of homeless people was found in the same cities.
Structural chaos cannot sustain clinical gains. Returning home with an eviction notice after spending 30 days in inpatient care, the system gets confused why they relapse a few weeks after. The majority of dual diagnosis care silently fails at this point. Not in the therapeutic setting, but in the space between it and the outside world.
What Integrated Care Has to Include
There are three things that separate dual diagnosis treatment from the one that looks good on paper.
A Unified Clinical Team
Firstly, your MAT prescriber, your trauma therapist, and your psychiatrist need to be at the same table. Evidence consistently shows that integrated, coordinated treatment for co-occurring diagnoses is usually better than parallel, uncoordinated services.
If your Suboxone doctor doesn’t know what your trauma therapist is working on, you get conflicting recovery goals. Medications get adjusted without context. Therapy sessions unpack things the prescriber doesn’t know about. You get confused. You get stuck. Therefore, a unified team means every clinical decision is made with the full picture, not just the piece of it that landed in one provider’s office.
Nervous System Stabilization Before Talk Therapy
A traumatized, dysregulated brain is not able to effectively process CBT or DBT. You can’t think your way out of a craving when your body is in survival mode. This is not a motivational issue. This is a physiology problem.
First, the somatic and trauma-informed work settles the physical storm so the mental work can fully land. Biofeedback teaches you how your own nervous system works, such as heart rate, muscle tension, and breathing patterns. This way you have real-time tools to help you bring it down before it takes over.
Trauma-informed breathwork does the same thing; it interrupts the stress response on a physiological instead of a cognitive level. You are not thinking yourself into calm. You are regulating your way to tranquility, which is a different mechanism entirely and a more reliable one when the brain is in a heightened state.
Hence, stabilizing the body first is not a sidetrack from real treatment. It’s what allows honest treatment to happen.
Case Management as Clinical Intervention
This is not a pamphlet about local resources. Not a referral list you get on discharge day. Instead, you receive active, hands-on coordination with housing navigation, legal support, and employment readiness all happening while you’re still in treatment.
Housing instability and pending court dates aren’t lifestyle inconveniences. They are serious relapse triggers, and treating them as an afterthought is the same as ignoring symptoms. Research on social determinants of health consistently shows that unstable housing is one of the strongest predictors of treatment dropout and relapse. This means that a person cannot focus on nervous system regulation in group therapy at 10 a.m. if they are terrified about where they are sleeping that night.
Good case management in a dual diagnosis program means someone is actively working those problems in parallel with your clinical care. That looks like coordinating with Rhode Island’s housing assistance programs, connecting you with legal aid for court navigation, and building an employment readiness plan that doesn’t assume you’ll figure it out after discharge. In Rhode Island, the structural pieces of your life are being addressed before you leave and are not handed to you as a to-do list on the way out the door.
The Step-Down Gap In Rhode Island And Surroundings
The 30-day residential program ends. The structure disappears. And for many Rhode Islanders, what follows is the loneliest and most dangerous part of recovery.
The leap from inpatient back to daily life is too steep without something in between. A real continuum looks like this: inpatient stabilization first, where the immediate crisis is addressed, and the nervous system has room to settle.
Then a partial hospitalization program (PHP), where intensive clinical support continues, but community reintegration starts. You practice being a person in the world again, in small doses. Then intensive outpatient (IOP), where peer support and regional mentoring networks take on more weight as the clinical structure gradually steps back. And throughout all of it, post-discharge planning that’s truly local matters. Crisis plans built around your specific neighborhood in Providence, Pawtucket, or wherever you’re going back to, not a generic aftercare template.
The scariest day of treatment shouldn’t be the day you leave.
Final Words
You don’t need to have all your ducks lined up before you call. You don’t have to know what level of care you need or how to explain what has been going on. That’s what the first conversation is for.
Rhode Island Addiction Treatment Centers works with dual diagnosis. We verify your benefits before any commitment is made, and we help you understand what treatment can actually look like for your situation. Call us at 888.541.4028 or visit Rhode Island Addiction Treatment Centers online.